The more you understand about primary immunodeficiency (PI), the better you can live with the disease or support others in your life with PI. Learn more about PI, including the various diagnoses and treatment options.
Living with primary immunodeficiency (PI) can be challenging, but you’re not alone—many people with PI lead full and active lives. With the right support and resources, you can, too.
Be a hero for those with PI. Change lives by promoting primary immunodeficiency (PI) awareness and taking action in your community through advocacy, donating, volunteering, or fundraising.
Whether you’re a clinician, researcher, or an individual with primary immunodeficiency (PI), IDF has resources to help you advance the field. Get details on surveys, grants, and clinical trials.
Variants in the genes encoding cytotoxic T lymphocytic antigen-4 (CTLA4) and lipopolysaccharide responsive beige-like anchor (LRBA) can cause immune dysregulation. This means the components of the immune system regulating inflammation, autoimmunity, and cancer lose their proper function, leading to an array of autoimmune disorders and infections.
Overview
CTLA-4 haploinsufficiency is a genetic condition in which one copy of the CTLA-4 gene is lost, leaving a single functional copy of the gene. However, having only one copy of the gene is not sufficient to produce normal function for the CTLA-4 gene in question.
LRBA deficiency causes poor immune function that results from uncontrolled activation and inadequate regulation of some immune cells. This results in both immune deficiency and immune dysregulation, the latter leading to a variety of autoimmune disorders.
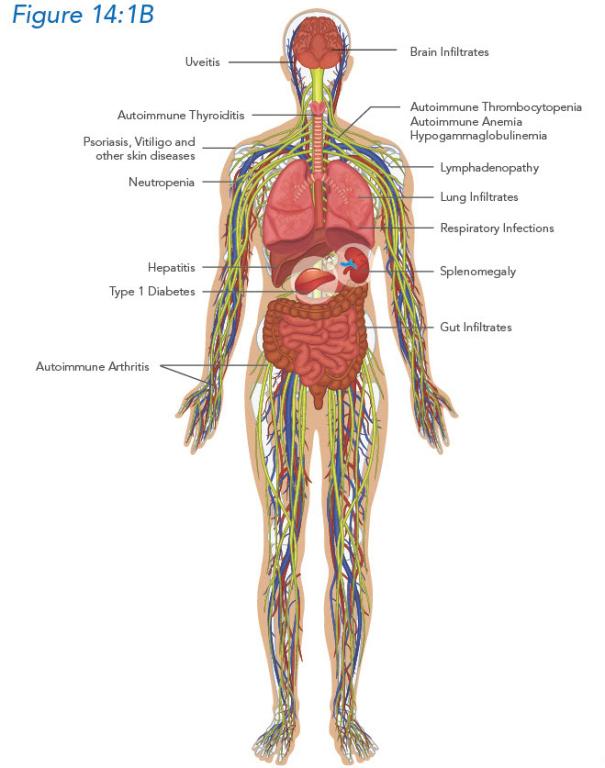
As a result, individuals with either of these diseases may have recurrent respiratory infections that start early in childhood, significant immune inflammation of their organs, and may have a number of autoimmune conditions. Autoimmune conditions occur when the immune system creates antibodies that attack the body’s own tissues and cells. There may also be an invasion of tissues with lymphocytes that result in the destruction or dysfunction of the targeted organs. The lungs, brain, intestines, liver, and kidneys are the organs most commonly affected. Uncontrolled aggregation of immune cells can lead to an enlarged spleen or lymph nodes. Additionally, because of immune dysfunction, these conditions increase the risk of developing some cancers, like lymphoma.
Immunobiology
The CTLA-4 protein, found on the surface of T cells, is critical for the immune system, particularly in the role of regulating and keeping the immune cells in check. The LRBA protein is important for the control and transport of CTLA-4 from inside the cell to the surface. Variants in either the CTLA-4 or LRBA genes may lead to significantly diminished or absent CTLA-4 protein and function, ultimately causing uncontrolled inflammation and autoimmunity.
Chapter 14: CTLA-4 Haploinsufficiency and LBRA Deficiency
Because variants in CTLA-4 and LRBA can both result in decreased CTLA-4 protein and function, there are many similarities in the clinical presentation of these two conditions. The hallmark feature of both is uncontrolled immune activation, inflammation, and often immunodeficiency.
Hypogammaglobulinemia, most commonly low IgG and low IgA.
Poor vaccine response.
Low circulating lymphocyte numbers, many with low B cells and T cells.
Low natural killer (NK) cells.
Low Treg cells.
The immunodeficiency is similar to common variable immune deficiency (CVID) as individuals have hypogammaglobulinemia and impaired antibody responses. In fact, some individuals with these conditions are initially diagnosed with CVID. Like individuals with CVID, they are prone to developing recurrent sinus and lung infections. These infections often start in childhood and can become more severe with age.
Individuals with LRBA deficiency usually present in their preschool age years, while those with CTLA-4 haploinsufficiency may not present until young adulthood. In both diseases, individuals also have increased susceptibility to infections caused by Epstein-Barr virus (EBV, the mono virus) and cytomegalovirus (CMV). These infections may recur frequently and may lead to the development of certain lymphomas.
Click to enlarge.
The degree of immune dysregulation, such as autoimmunity and inflammation, seen in individuals with CTLA-4 haploinsufficiency and LRBA deficiency is clinically quite variable. Both diseases may present with chronic diarrhea caused by inflammation of the intestine, also called enteropathy. An individual may present with failure to thrive, weight loss, or nutritional deficiencies because of chronic gastrointestinal losses.
Almost all individuals will develop an autoimmune condition as part of their immune dysregulation at some time in their lives; some individuals develop multiple autoimmune problems. Autoimmune conditions result from the body making antibodies that attack the body’s own tissues and cells. Autoimmune cytopenias (low white blood cells, red blood cells, or platelets) are the most common issue. Individuals can also form antibodies that attack their own organs (such as the thyroid, pancreas, and joints) and result in the destruction and altered function of those organs or tissues. This may present in the form of thyroid disease, diabetes, arthritis, psoriasis, vitiligo, or alopecia (hair loss). Similarly, some individuals develop aggregates of immune cells or lymphocytes that appear as localized areas of inflammation in their vital organs and lead to organ dysfunction. In CTLA-4 and LRBA, the most often seen type of inflammation occurs in the lung, brain, intestines, bone marrow, and—to a lesser degree—in kidneys.
On clinical exam, individuals with CTLA-4 haploinsufficiency or LRBA deficiency may have a big spleen, liver, or sometimes enlarged lymph nodes.
Individuals with CTLA-4 haploinsufficiency and LRBA deficiency are at increased risk for developing cancers and lymphoma. Because of this, their health status needs to be closely monitored.
Find CTLA-4 haploinsufficiency and LRBA deficiency clinical trials
See if you qualify to participate in clinical trials evaluating new treatments and/or diagnostics for CTLA-4 haploinsufficiency or LRBA deficiency.
CTLA-4 haploinsufficiency or LRBA deficiency should be considered in any individual who presents with early-onset recurrent sinopulmonary infections and autoimmune conditions. The symptoms can include chronic diarrhea, weight loss or failure to gain weight, an enlarged spleen, and/or enlarged lymph nodes. White blood cell infiltration of certain body parts (such as the lung, brain, kidney, intestines, or bone marrow) is also a distinguishing feature of both diseases.
When considering CTLA-4 or LRBA variants as a potential cause of disease in an individual, an initial immune evaluation should include a complete blood count (CBC) with differential to look for low blood counts, serum immunoglobulins (IgG and IgA are usually low, while IgM can be normal or low), and flow cytometry to look at the numbers of different kinds of lymphocytes. Individuals may not have protective levels of antibodies, even to diseases against which they have been vaccinated. Autoimmune conditions are often diagnosed by detecting auto-antibodies, or antibodies targeted at the body’s own tissues and cells. When there is a clinical concern for lymphocytic infiltration of organs, imaging studies (usually CT scans or MRIs) or even biopsies of these tissues may be necessary.
Ultimately the diagnosis of CTLA-4 haploinsufficiency or LRBA deficiency is confirmed after identifying a gene variant with genetic testing.
Read the latest research
Read the latest research on CTLA-4 haploinsufficiency and LRBA deficiency on PubMed. Note that not all publications listed in PubMed are freely available; some require a subscription to the publishing journal.
Both CTLA-4 haploinsufficiency and LRBA deficiency are rare immunologic diseases that can be inherited or passed on to family members, or they can occur spontaneously. CTLA-4 haploinsufficiency is caused by a variant in one copy of the CTLA-4 gene, resulting in decreased protein and function. The inheritance pattern for CTLA-4 haploinsufficiency is known as autosomal dominant, which means that if a child inherits the gene variant, the child can have the disease. The chance of a child inheriting the variant is 50% if one of the parents carries it. Some individuals with CTLA-4 haploinsufficiency appear to be asymptomatic, meaning they have the variant but have no clinical signs of the disease. This is because CTLA4 haploinsufficiency is considered to have variable penetrance. As a result, multiple members of the family may carry the gene variant but only some may be sick, and some may not be sick at all. Nonetheless, all family members identified with the variant need to be counseled about their risks, as disease signs and symptoms can present later in life.
LRBA deficiency is usually caused by two copies of the LRBA gene with variants causing decreased protein. The inheritance pattern for LRBA deficiency is known as autosomal recessive, meaning that both gene copies must have the variant for the condition to develop. The chance of a child inheriting the condition is 25% if each parent is a carrier of one variant. Unlike CTLA-4 haploinsufficiency, LRBA deficiency has shown near complete penetrance, meaning that people with the two variants (one in each copy of the gene) almost always have clinical signs of disease.
Treatment
Individuals with CTLA-4 haploinsufficiency or LRBA deficiency who have recurrent infections because of an antibody deficiency require immunoglobulin (Ig) replacement therapy. They may be treated with prophylactic antibiotics, which are antibiotics given to prevent the development of disease or infection. The goal of these therapies is to prevent organ damage from frequent infections.
Individuals with evidence of significant immune dysregulation and resulting decreased organ function should be treated with immune suppression. These therapies work to turn off the dysregulated immune system. There is now an injectable drug, abatacept, a medication approved by the FDA for use in rheumatoid arthritis and certain types of psoriasis, which can act as a CTLA-4 replacement. It has shown promising results in improving the immune dysregulation in both individuals with CTLA-4 haploinsufficiency and LRBA deficiency.
Other immunosuppressants often used to treat these diseases include systemic steroids (such as prednisone, methylprednisolone), sirolimus, and rituximab. Sirolimus is an immune suppressant that inhibits the activation of T cells and B cells, useful in preventing the rejection of kidney transplants. Rituximab is a monoclonal antibody directed at B cells and is used to treat a number of autoimmune diseases and certain cancers. As with many primary immunodeficiencies, hematopoietic stem cell transplantation (HSCT) is an option in treating CTLA4 haploinsufficiency and LRBA deficiency but has significant risks.
Expectations
Some people carrying CTLA-4 variants do not have signs or symptoms of disease or may be minimally affected (for example, they may only have thyroid disease or vitiligo). Still, they must be followed closely by doctors because they are at risk for developing more signs and symptoms of disease later in life.
Once on appropriate management to reduce infections, inflammation, and autoimmunity, many individuals with CTLA-4 haploinsufficiency or LRBA deficiency are able to lead relatively normal lives. They do not need to be isolated or limited in their daily activities. Because the types and extent of immune dysregulation seen in both CTLA-4 haploinsufficiency and LRBA deficiency are quite variable, individuals often are followed by many subspecialty doctors and need close monitoring.
This page contains general medical and/or legal information that cannot be applied safely to any individual case. Medical and/or legal knowledge and practice can change rapidly. Therefore, this page should not be used as a substitute for professional medical and/or legal advice. Additionally, links to other resources and websites are shared for informational purposes only and should not be considered an endorsement by the Immune Deficiency Foundation.